
LAS VEGAS — Obamacare, the politicians of America and Nevada are discovering, is a realm of the “unknown unknowns.”
The phrase comes from a former U.S. secretary of defense who once publicly distinguished the “known unknowns“— the things we currently know we don’t know — from the unknown unknowns: the things we currently are not even aware that we don’t know.
Case in point: the long and growing list of questions the Obama administration appears incapable of answering today about its signature legislation, the Patient Protection and Affordable Care Act, in the wake of the June 28 U.S. Supreme Court rulings.
Tuesday, Virginia Gov. Bob McDonnell, representing the public policy committee of the Republican Governors Association, wrote U.S. Health and Human Services Secretary Kathleen Sebelius for the second time.
He was requesting answers to 30 basic questions governors have about the implementation of Obamacare’s health-insurance exchanges and expansion of Medicaid, following the Supreme Court’s rewrite of PPACA to make it arguably constitutional.
“As you may have seen from the reports from the National Governors Association meeting … ,” wrote McDonnell, “a majority of the nation’s governors are uncertain about the major decisions which must be made on what kinds of exchanges to implement, whether to expand Medicaid, and how the vast new bureaucracies will be paid for and administered in a nation $16 trillion in debt.”
McDonnell said that his first letter — requesting answers to 17 questions regarding health exchanges and 13 questions regarding Medicaid — had only elicited from the Obama administration “a cordial but vague response,” which was “wholly inadequate” given “the challenging and detailed work ahead for our nation…”
Here in Nevada tomorrow, the state’s governor, secretary of state and attorney general — holding hands, as it were — are scheduled to take a big step together into that uncharted realm of unknown unknowns, drawing the people of Nevada in behind them.
Meeting as the state Board of Examiners, the three constitutional officers are being asked by the board of the Silver State Health Insurance Exchange (SSHIE) to approve a $72 million, four-and-a-half-year contract with Xerox Health Care Solutions, LLC, to provide and maintain a web- and telephone-based “Business Operation Solution (BOS)” call center to implement Obamacare’s plan for health care in Nevada.
Eleven days earlier, the same proposal had been on the Board of Examiners agenda although it had not yet been approved by the SSHIE board. At that point, the clerk of the BoE opted to pull the item and send it back to the SSHIE board.
On Thursday evening, in a special telephonic call-in meeting arranged for the specific purpose of ratifying the contract, the SSHIE board endorsed it.
One board member — Dr. Ronald J. Kline, of the Comprehensive Cancer Centers of Nevada — asked whether, given the $72 million cost of the contract, the state should not perhaps own, rather than merely lease, the software behind the BOS.
The answer he was given, he told Nevada Journal, was “that to own it would be much more expensive.”
Moreover, Kline said, “Their response was that the $70 million … was less than any other state by a factor of two, if I remember correctly.” Later, he added, “I don’t think there’s anything nefarious here. I mean, I don’t know the cost of these programs. If it was $72 million to lease it and $73 million to buy it, I’d say buy it. But my understanding is, that in comparison to other states, this is half the cost of other states, so in that sense it seems like it actually makes sense.”
However, a contract described on Xerox’s own website would appear to possibly contradict the response given Dr. Kline:
DALLAS – Florida Health Choices, a corporation established by the state to improve access to health care, has selected Xerox (NYSE: XRX) to administer its Insurance Marketplace, a program designed to give small business and eligible individuals more flexibility in finding affordable health insurance and other services. The nine-year contract is valued at $68 million. (Emphasis added.)
One member of the public attending the SSHIE board’s telephonic meeting later expressed concern that the board and its staff may be rushing to spend taxpayer dollars without performing adequate due diligence.
The State of Nevada “will never be in a stronger position than we are right now to negotiate the most favorable terms,” said Brent Husson, of Employee Benefit Management Services of Nevada, “and we are letting this slip by.
“The ongoing cost of administering the exchange is what will end up being the biggest ticket item in all of this. Right now Xerox is going to charge about $7.30 per member per month, which will be a couple million per month. However, when the contract goes to bid, another company will have to charge well over that amount in order to make up for the cost of developing a new platform, or integrating into the existing one.
“Xerox will know this and be able to raise their fees to just under that amount. The bottom line is that there could be language put into the contract now that would protect Nevada from this, but I do not see that anyone has considered doing it.”
Nevada appears to be the single state with a Republican governor that is actually seeking to actively move ahead with implementation of an Obamacare-compliant health insurance exchange, according to data compiled by PoliticoPro.com and Nevada Journal.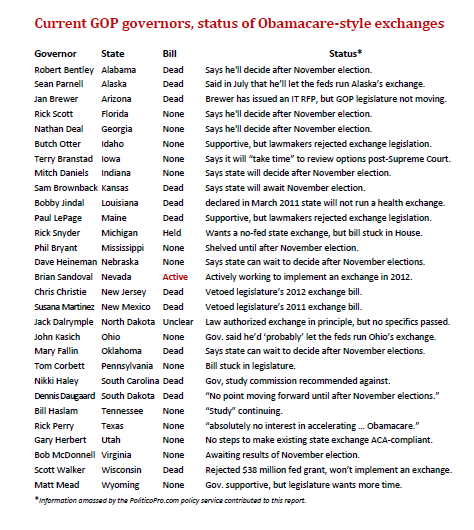
While a handful of GOP governors have expressed some support for the idea of state-only health-insurance exchanges, their legislatures, almost universally, have declined to go along.
Most Republican governors, by far, have indicated that they will postpone any decision until after the November elections, which they expect should clarify matters greatly. Should presumptive Republican presidential nominee Mitt Romney win the White House, he has pledged to end Obamacare virtually his first day.
Even if Romney does not win, however, some of the governors have said, the additional time itself should allow more clarity to emerge.
Many governors cite the current absence of answers to their many questions about the health insurance exchanges and the Medicaid expansion.
“It doesn’t make sense to spend Alaskans’ dollars to set up an exchange when so much uncertainty exists about how to implement it and how to gain federal approval,” Alaska Gov. Sean Parnell said in July.
In New Jersey, Gov. Chris Christie vetoed the legislature’s exchange bill in May and says, given the uncertainty, he would veto it again if it came up before November.
Ohio Gov. John Kasich has said he’d probably let the feds run Ohio’s exchange, but is pressing the feds for more guidance on exchange requirements, including the partnership model and the federally facilitated exchange. Lt. Gov. Mary Taylor, who is also the state’s insurance commissioner, cites state projections that an exchange would only increase premiums in the state. “Obamacare is wrong for Ohio,” she has stated.
South Dakota Gov. Dennis Daugaard said in January that that state won’t try to pass legislation this year to set up an exchange. Even after the Supreme Court ruling, he says, the elections are creating so much uncertainty that there’s no point in moving ahead.
In Texas, Gov. Rick Perry — whom Sandoval initially supported for the GOP presidential nomination — has made it emphatically clear he “has absolutely no interest in accelerating the implementation of Obamacare,” a spokesperson said, and will not create a health insurance exchange before the November elections.
In Virginia, McDonnell, following the Supreme Court rulings, said his state needed more information about the federal exchange before deciding anything. State lawmakers, at his request, have delayed legislation to actually establish any state-based exchange.
Wisconsin Gov. Scott Walker in January turned down a $38 million “Early Innovator” federal grant and — declaring the state won’t implement an Obama-compliant exchange — has called off all planning activities. However, Wisconsin may endorse a self-funded, privately run exchange, Walker has stated.
Following the Supreme Court ruling, state policymakers across the U.S. are finding that Obamacare, as Cato health-care analyst Michael Tanner puts it, is now a “bigger mess” than ever.
He notes that — now that “Congress can’t strip all Medicaid funds from states that refuse the [Medicaid] expansion, as the ObamaCare law threatened” — responsible state policymakers face a genuine dilemma:
If they agree to expand their Medicaid programs anyway, they’ll be choosing to pile new costs on their state budgets and new taxes on their constituents.
And if a state doesn’t expand its Medicaid program, most of those who would’ve been eligible for Medicaid will now become eligible for subsidies through Obamacare’s health-insurance exchanges. And those subsidies are paid in full by the feds … [which] will cause the federal cost of ObamaCare to skyrocket.
If every state were to refuse to expand its Medicaid program, notes Tanner, federal costs would go up at least $100 billion a year — on top of the more than $823 billion that Obamacare will add to the federal deficit, under estimates that assumed state taxpayers would be picking up some Medicaid costs.
“How will Congress react if billions or perhaps trillions of dollars in new costs are added to the federal budget?” asks Tanner.
“In short,” he says, “the Supreme Court’s ruling not only guaranteed that ObamaCare will be an issue in this fall’s federal elections; it dumped a mess in the laps of governors and state legislators, too.”
Jon Hager, executive director of SSHIE, regularly argues that Nevada, however, should press quickly ahead.
“The problem with putting it off until after the election,” he told Nevada Journal, “is that it won’t give us enough time to implement it by the deadlines. The way the deadlines are written right now, I believe, we have until the middle of November to submit our blueprints and a declaration whether or not we’re going to implement an exchange.”
Nevada has “until January first of next year, 2013, to get certified” as Obamacare-compliant by the federal Centers for Medicare and Medicaid Services, while facing a current federal deadline for open enrollment by Oct. 1, 2013.
“The project is so complicated that to be able to start in November and have everything done in 11 months is unrealistic,” he said.
Hager contended that Nevada will gain important “flexibility” by quickly establishing an Obamacare-compliant health-insurance exchange — although he acknowledged that “basically state law says that we are going to follow federal law,” defined as including any amendments to the law and any “guidance” the federal government chooses to issue in the future.
Examples of such permitted flexibility, he suggested, include:
- Allowing the state to set up its own Navigator program,
- Allowing the state to decide whether or not to allow brokers to sell products in the exchange,
- Allowing the state to “set up our own web portal, with potential links to businesses in Nevada, rather than some product that the feds provide,”
- Allowing the state to make decisions regarding “our essential health benefits,”
- Allowing the state to make “decisions regarding the reinsurance and risk-adjustment programs.”
Another important consideration Hager offered is that doing a state-based exchange “is allowing us to … have dialogue with the federal government on what works and what doesn’t. And what could harm the Nevada market and what may not.
“And so that would allow us to influence the regulation-making process. If we’re not part of that conversation, if we just say, ‘You know what, the feds are going to run it,’ they could implement regulations that substantially harm the market. And so, one of our goals is to mitigate the risks that may be created by harmful regulations. By being part of that dialogue, we have the chance to provide input to those regulations.”
In actuality, assert policy analysts at the libertarian Cato Institute and the conservative Heritage Foundation, “the promise of local control” over Obama-compliant health-insurance exchanges “is a mirage.”
Testifying before the New Hampshire legislature, Cato analyst Michael Tanner noted that “The law allows the federal government to commandeer any state-run Exchange that falls short of full compliance with federal dictates.”
And, as Nevada Journal noted last week, the same provisions are — following the 2011 Legislature — implicit in Nevada law, since section 1321(c) of the Affordable Care Act “authorizes HHS (1) to ensure that States with Exchanges are substantially enforcing the Federal standards to be set for the Exchanges and (2) to set up Exchanges in States that elect not to do so or are not substantially enforcing related provisions.” (Emphasis added.)
Tanner also noted that “The conservative Heritage Foundation once took the position that states should set up a ‘defensive’ Exchange to preserve a modicum of control over their Medicaid programs. After reading the administration’s Exchange regulations and concluding that the federal government will allow state-run Exchanges no such autonomy, Heritage scholars now counsel states to refuse to establish one of the law’s Exchanges and to send all related grants back to Washington.”
The federal government will “heap regulations upon state-run Exchanges,” said Tanner. “Indeed, it is already imposing greater requirements on them than the law itself does.”
Creating a state-run exchange, Tanner told New Hampshire lawmakers, “would not prevent a federal takeover of New Hampshire’s health insurance markets, it would lend manpower to that effort.”
After listening to Tanner, New Hampshire lawmakers sent a $1 million planning grant back to the federal government in 2011 and passed a bill in June blocking the state from running its own exchange.
Steven Miller is the managing editor of Nevada Journal, a publication of the Nevada Policy Research Institute. For more in-depth reporting, visit https://nevadajournal.com/ and http://npri.org/.